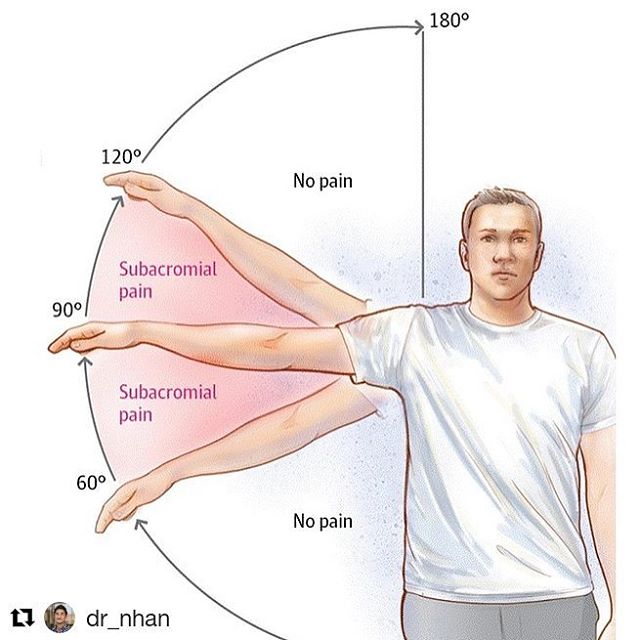
@dr_nhan (@get_repost)・・・Shoulder Impingement Syndrome (aka Subacromial Impingment): one of the most common conditions I see that result in shoulder pain. Most patients will complain of pain near the front or side of the shoulder with very particular arm movements, usually involving flexion and/or abduction of the glenohumeral joint along with certain degrees of internal and external rotation. Some may experience referral pain on the side of the arm or even down near the elbow, thinking it&;s elbow pain.Anatomically, when the arm is lifted into these painful ranges, the structures between the humerus and acromion (what we call the subacromial space) have the potential to get pinched. These structures may include the supraspinatus tendon, biceps tendon, subacromial bursa, and subscapularis tendon. The reason this pinch occurs is most commonly due to less than optimal biomechanical movement – the most common being scapular instability, scapular dyskinesis, and poor rotator cuff engagement or sequencing. Hence, if you attempt to move the shoulder without proper shoulder stability or muscle firing patterns, the humerus can ride up too close to the acromion which causes the structures in the subacromial space to pinch underneath the acromion. Thus, to mend these issues one must train the muscles that stabilize the scapula and the rotator cuffs muscles to function appropriately. My shoulder protocol of choice for these cases involve training the serratus anterior with high plank protractions, rhomboids with rows, subscapularis with internal rotations, infraspinatus and teres minor with external rotations, and posterior deltoid with horizontal abductions. You can refer to the last four exercise videos on this page for demos on variations of these exercises. This protocol is also a great prehab warm up routine that I personally use before my upper body days in the gym, which can help PREVENT shoulder impingement from even occurring. Feel the gains to prevent the pain

Comments are closed.