She came in today with some headaches and the left side of her neck jacked up and unable to turn left to shoulder check! Today we worked A few ART soft tissue passesNeck traction and mid back adjustingReleasing the root cause – posted on October 4, 2017 by Dr. Jonathan Leung | No comments
Patient of mine working as a machine operator with tennis elbow or lateral epicondylitis on BOTH arms!Treated him using Instrument Assisted Soft Tissue ARTWrist and elbow magicEccentric exerciseThis is the best I could ask for from this fine gentleman.Some of you climbers and dodgeballers get some of this elbow pain. Check yourself before you wreck yourself. posted on September 29, 2017 by Dr. Jonathan Leung | No comments by
Starting up some new programming as suggested by a patient of mine. Reminding me of the days we used to lift in the school gym together. Even though we may all have our own challenges now we can still push each other up and grow from the struggle. @hk.rehab@philio10@geotran32 @mpchiropractic @primewayoflife (@get_repost)・・・Embrace the struggle, let it make you stronger posted on September 27, 2017 by Dr. Jonathan Leung | No comments by
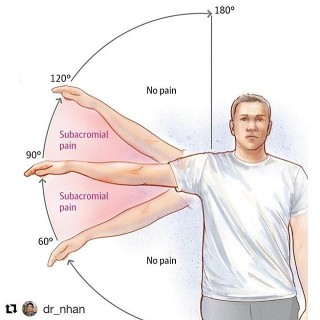
This is the Hawkin&;s kennedy test – it&;s an orthopaedic test designed to be coupled with a few other tests in order to test for subacromial impingement – often coupled with the painful arc and an infraspinatus test.To try this – keep the upper arm parallel to the floor, and rotate the forearm inwards towards the ground, you can do this at various angles as you move the arm across the body.Either try this yourself or have someone try this on you. If it hurts you may have some sub-acromial impingement! Ask yourself: Do I do a lot of repetitive overhead movements?Does it hurt when I throw right in the front point of the shoulder?Do I avoid certain movements because it hurts or feels awkward?Do I favor one side over the other because of this?Book an assessment with a professional as there are plenty of factors that can contribute to this. To name a few: Weak rotator cuff musclesTight rotator cuff musclesImproper glenohumeral rhythmPoor movement patternsThoracic spine limitationsSICK scapula posted on September 25, 2017 by Dr. Jonathan Leung | No comments by
@dr_nhan (@get_repost)・・・Shoulder Impingement Syndrome (aka Subacromial Impingment): one of the most common conditions I see that result in shoulder pain. Most patients will complain of pain near the front or side of the shoulder with very particular arm movements, usually involving flexion and/or abduction of the glenohumeral joint along with certain degrees of internal and external rotation. Some may experience referral pain on the side of the arm or even down near the elbow, thinking it&;s elbow pain.Anatomically, when the arm is lifted into these painful ranges, the structures between the humerus and acromion (what we call the subacromial space) have the potential to get pinched. These structures may include the supraspinatus tendon, biceps tendon, subacromial bursa, and subscapularis tendon. The reason this pinch occurs is most commonly due to less than optimal biomechanical movement – the most common being scapular instability, scapular dyskinesis, and poor rotator cuff engagement or sequencing. Hence, if you attempt to move the shoulder without proper shoulder stability or muscle firing patterns, the humerus can ride up too close to the acromion which causes the structures in the subacromial space to pinch underneath the acromion. Thus, to mend these issues one must train the muscles that stabilize the scapula and the rotator cuffs muscles to function appropriately. My shoulder protocol of choice for these cases involve training the serratus anterior with high plank protractions, rhomboids with rows, subscapularis with internal rotations, infraspinatus and teres minor with external rotations, and posterior deltoid with horizontal abductions. You can refer to the last four exercise videos on this page for demos on variations of these exercises. This protocol is also a great prehab warm up routine that I personally use before my upper body days in the gym, which can help PREVENT shoulder impingement from even occurring. Feel the gains to prevent the pain posted on September 22, 2017 by Dr. Jonathan Leung | No comments by
Little bit o deep squat for hip mobility in prep for another long bout of delays in the airport. Mobility time posted on September 10, 2017 by Dr. Jonathan Leung | No comments by
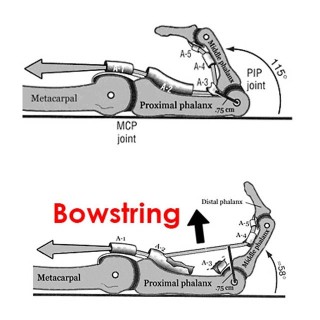
[Finger anatomy series 3/3] 3.The Proximal Interphalangeal joint or PIPNow that you know about the flexor tendons, the function of the pulleys and where they tend to pull, you should be able to guess why the PIP joint is so important!The PIP is the main joint that dictates the forces along the pulleys due to the position and angle of pull from the forces of the tendons.Demonstrated here is more of a hanging grip or an open handed grip. The angle of the PIP in this image is quite large and thus the resultant forces on the pulleys is minimal !! The SMALLER angle in the PIP = GREATER forces on the pulleys! Take this into consideration when thinking about how you grip your holds! I&;ll demonstrate with some more pictures in the following posts! posted on August 22, 2017 by Dr. Jonathan Leung | No comments by
[Finger anatomy series 2/3] 2. Annular Pulleys These puppies prevent your finger from doing something known as bowstringing. These pulleys are fibrous bands that are used to maintain the contact of the finger tendon along the bone. What they do is transmit the force of the tendon into different angles of pull. Without them our hands wouldn&;t function very well and would look very weird. Bowstringing occurs when there has been a COMPLETE pulley rupture. With climbing the A2, A4 and A3 are most commonly injured!A2 is the largest of them all and attaches directly to bone. This one takes the brunt of the work when we go to climb or crimp!A3 attaches to whats known as the volar plate – it doesn&;t really attach directly to the bone! This is super super important when ADOLESCENTS or younger adults are climbing as an injury here can PERMANENTLY affect a GROWTH PLATE! It can potentially cause dramatic issues for their future. A rule of is if an adolescent complains of finger injury – SEEK PROFESSIONAL HELP. A4 attaches to the bone directly as well closer to the finger tip and is much smaller than the A2. How can you use this to help? Put less strain on your pulleys! Warm up with progressive bodyweight when crimping. Slow and steady wins the race. Feel free and content with any questions or concerns but up next is the PIP and how to crimp safer and stronger! posted on August 18, 2017 by Dr. Jonathan Leung | No comments by
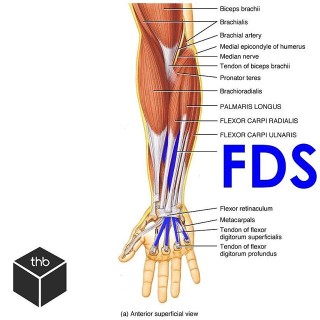
1. Flexor tendonsThe flexor tendons in the fingers occur because the muscles of the forearms become tendons as they enter the carpel tunnel into the hand.As you can see from the first image we have a bunch of other muscles of the forearm that affect motion of the hand and wrist. Well ignore those for now! First up is the Flexor digitorum superficialis or FDS. Swipe ️ and see it visualized again with its interaction with its deeper counterpart. The Flexor digitorum profundus or FDP is the deeper muscle that extends to the finger tip and helps us with flexing the entire fingerFDS is a tendon that splits into a V to allow the deeper FDP to run between it right to the tip! It inserts into the middle phalanx and flexes primarily the PIP joint. The design of these two tendons contribute to why we have such fine motor control at our fingers but it&;d be a shame if these tendons didn&;t have anything strong to hold them down! Next up. Pulleys. posted on August 17, 2017 by Dr. Jonathan Leung | No comments by